Many Autistic Children Have Speech Delays That Persist Despite Intervention
Autistic children are often speech delayed. These delays persist to an extent strongly related to their progress in the first 5 years of life[1]. There are behavioral interventions known to improve speech outcomes in this population. They generally focus on improving joint attention, play skills, gestures, and vocalizations[2]. However, many children despite receiving these interventions remain delayed. More is needed.
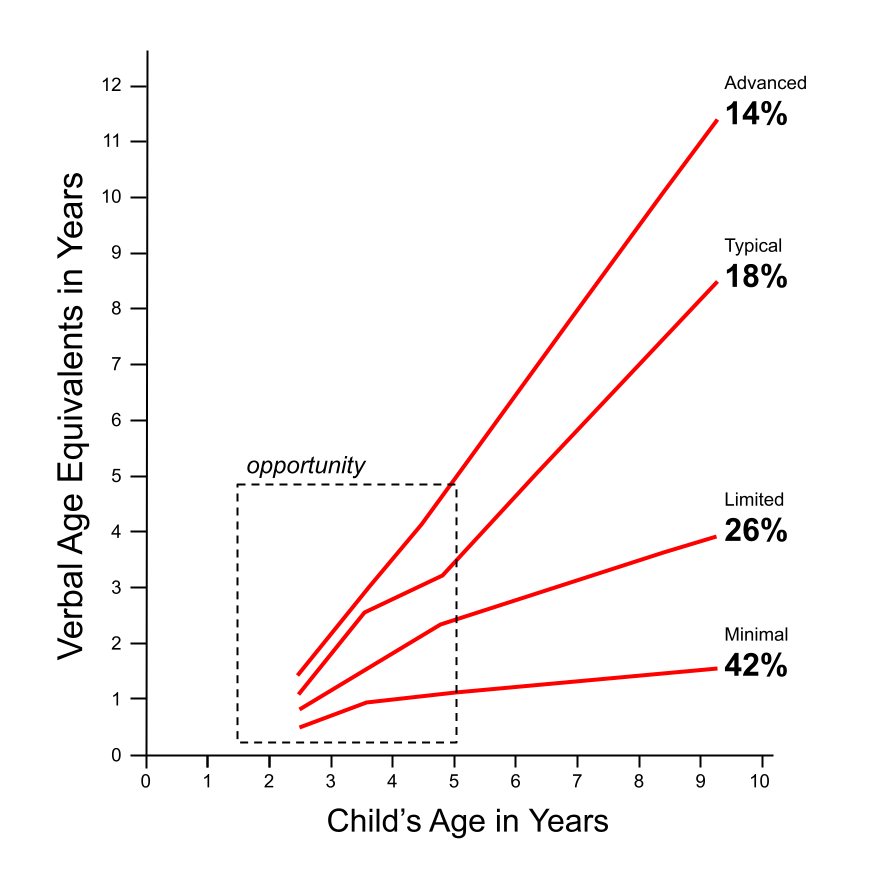
Figure 1: Speech development trajectories showing different outcomes (Advanced 14%, Typical 18%, Limited 26%, Minimal 42%) related to early progress[1].
Speech Generating Devices Can Help Develop Natural Speech
A speech generating device (SGD) is a grid of words represented by picture symbols that talk when pressed. It is often called "high tech AAC" or just "AAC." They are used as a communication system by non-speaking or minimally verbal individuals.
In 2014, Kasari et al[3] performed a randomized control trial on 61 minimally speaking autistic children ages 6-8. This is an age where new speech acquisition is typically considered challenging. They found that introducing an SGD on top of a behavioral intervention significantly (50%) increased the frequency of natural speech. This result is a remarkable confirmation of an observation that has been anecdotally reported previously — that a tool for nonverbal communication could boost natural speech output.
A Contrast Between Ways of Using Speech Generating Devices
The finding of Kasari et al might seem to be supportive of the notion that introducing SGDs is a "killing two birds with one stone" practice. It provides relief to a speech-delayed child's communication frustration, while simultaneously raising the likelihood of developing natural speech. However, a closer examination reveals key differences in the way an SGD was used in the study, and the way SGDs are typically introduced to children today.
In Kasari's study, the SGD was used for >50% of the interactions in a free-flowing play-based behavioral intervention. Thus the priority was on using high interest "fringe" words with easy navigation and accessibility. Toward this end, they used a grid of <16 words relevant to the activity — mainly nouns — that were organized into a single grid.
In contrast, when SGDs are introduced as a system for nonverbal communication, the emphasis is on teaching a child to navigate through a robust system containing tens of thousands of vocabulary words and their corresponding picture symbols. This goal is aligned with the expectation of lifelong use, and congruent with vocabulary growth in typically developing children. Out of necessity, these words are organized into multiple hierarchical pages. Much emphasis is placed on providing enough repetition and practice so that the child develops a motor plan enabling them to access these words with automaticity. Current SGD software, e.g. Proloquo, Touchchat, and LAMP, have evolved toward this end.
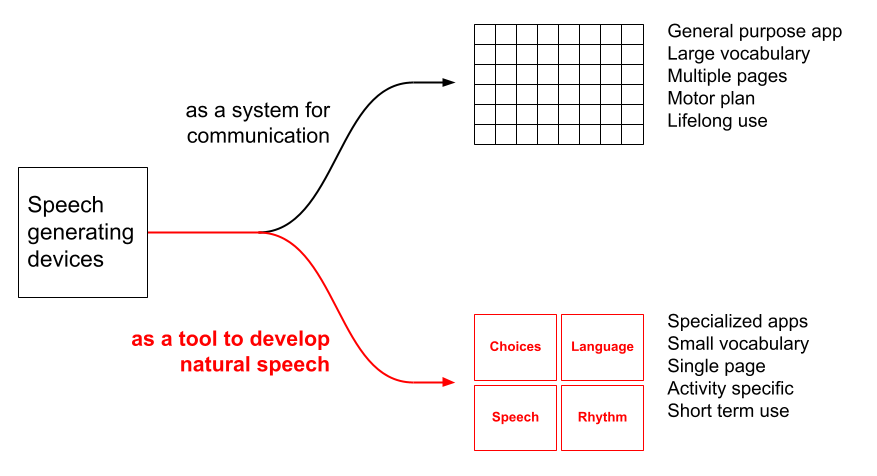
Figure 2: Contrasting approaches to using speech generating devices: as a communication system versus as a tool for developing natural speech
In Kasari's study, introducing an SGD had a powerful knock-on effect on natural speech production. However, their use of the SGD was very different from the way SGDs are currently used. Given this difference, it is reasonable to conclude that SGDs designed solely to improve the production of natural speech — and freed from the constraint of acting as a tool for all communication — would look very different than systems currently used today. Such systems would not preclude or replace use of existing SGD software. Instead, they would serve as a powerful complement and reassurance to families that "no one is giving up on speech." We discuss the design and implementation of such speech boosting systems in the next section.
The Approach: Multiple Apps Targeting Natural Speech Improvement
Three guiding principles apply to the development of speech boosting software. First is the primacy of tappable speaking tiles. SGDs are thought to exert their positive influence on natural speech through three broad mechanisms: raising the frequency of communication, reducing motor effort, and stimulating brain areas responsible for language[4]. So that this continues to apply, the apps must use speaking tiles that are both rewarding and easy to tap, and that trigger some learning when tapped.
Second is the need for multiple apps targeting different deficits in different domains. In 2023, NIH held a workshop[5] on "Minimally Verbal/Non-Speaking Individuals With Autism: Research Directions for Interventions to Promote Language and Communication." A key consensus was that this population is incredibly heterogeneous. Every child is minimally verbal or non-speaking for different reasons, and no single intervention is universally effective. On the technology end, a single app would be hard pressed to address equally well deficits in — for example — language cognition versus oral-motor coordination. A follow up conversation with an NIH program manager led to her observation: "you need an app that could let you rapidly trial multiple conditions ... you almost need multiple apps." We concur. A collection of specialized apps — accessible in cost and with generous trial capability — would enable a clinician to "dial in" a therapy individualized to a child's unique profile.
Third, each app must build on an evidence-based method. More details below.
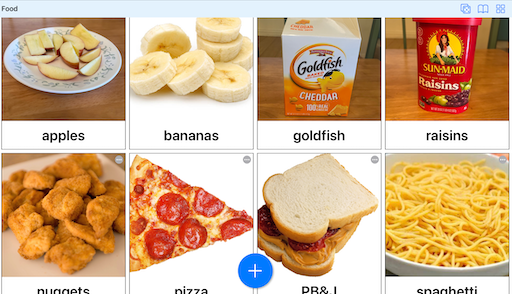
Visual Choices
Makes it easy to create instant photo boards, and is being used as an SGD in Prof. Kasari's autism intervention group at UCLA to good effect.
Evidence-based Method: Aided Language Stimulation in an SGD with a minimal grid (<16 words) of words relevant to a play activity.
Trial: 30 days free OR use Lite Mode indefinitely (5 items, 1 board)
Cost: $5/month

Visual Language
Combines explicit language instruction with a "magic AAC" that has a grid of nouns, verbs, adjectives, and prepositions, and provides instant picture feedback.
Evidence-based Method: Aided Language Stimulation in an SGD with explicit inclusion of nouns, verbs, adjectives, and prepositions in a single-page grid.
Trial: Use Lite Mode indefinitely (max 2 word sentences)
Cost: $25 one time
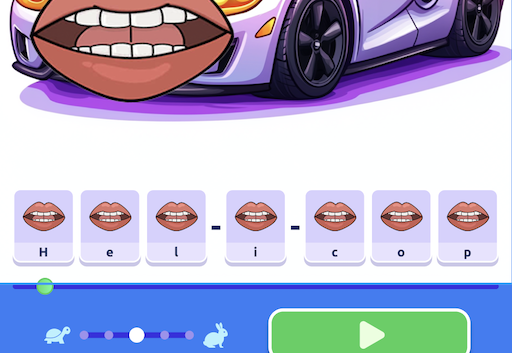
Visual Speech
Provides visual and auditory cues through animated cartoon lips superimposed on objects of interest. Words are broken apart into tappable phonemes.
Evidence-based Method: Dynamic Temporal and Tactile Cuing (DTTC) uses visual, auditory, and tactile cues to teach motor movements, with immediate feedback.
Trial: 30 days free OR use Lite Mode indefinitely (5 items, 1 board)
Cost: $5/month
In development
Visual Rhythm
Turns Auditory Motor Mapping Training into a fun rhythm game. Children tap on picture tiles of key words or syllables in favorite songs.
Evidence-based Method: Auditory Motor Mapping Training, a method where a child and clinician tries to sing two syllable words together, while the child drums in time with the sung syllables.
Trial: Use Lite Mode indefinitely (one song)
Cost: $25 one time
In development
The Need for Community Involvement
Good software is a conversation, not an edict. The above represents an initial release. We wish to continue development with strong input from the community, particularly feedback from use with children. Speech therapists, assistive technology specialists, applied behavioral analysts, early interventionists, special education teachers, parents, and others are approaching a common goal from diverse perspectives. Our desire is to create software that transcends ideological barriers and works for everyone. We believe that a person should not have to adapt to software; software should adapt to the person. Robust and ongoing community involvement will enable us to rapidly bridge the gap between what should work and what does work.
Natural Speech Is Best
It is fast — more than 150 words per minute versus 15 words per minute for an average SGD user[10]. It is unconstrained — a speaking person can build an unlimited vocabulary around their needs and interests, and pick the right words without limits. They can say what they want to say in their own voice. They can also say everything they want to say — more than 16,000 words per day versus 100 words per day for an average SGD user[11].
It is attainable. In Kasari's study, minimally verbal children ages 6-8, most of whom had gone through years of interventions, began to talk, even more so when SGDs were used in the session. What is needed are behavioral interventions supported by decades of evidence, combined and integrated with technology that is now emerging, developed iteratively with the strong input of the community. We need your help. Will you join us?
References
[1] Anderson, D. K., Lord, C., Risi, S., DiLavore, P. S., Shulman, C., Thurm, A., Welch, K., & Pickles, A. (2007). Patterns of growth in verbal abilities among children with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 75(4), 594-604.
[2] Kasari, C., Paparella, T., Freeman, S., & Jahromi, L. B. (2008). Language Outcome in Autism: Randomized Comparison of Joint Attention and Play Interventions. Journal of Consulting and Clinical Psychology, 76(1), 125-137.
[3] Kasari, C., Kaiser, A., Goods, K., Nietfeld, J., Mathy, P., Landa, R., Murphy, S., & Almirall, D. (2014). Communication Interventions for Minimally Verbal Children With Autism: A Sequential Multiple Assignment Randomized Trial. Journal of the American Academy of Child & Adolescent Psychiatry, 53(6), 635-646. Clinical trial registration: NCT01013545.
[4] Blischak, D. M., Lombardino, L. J., & Dyson, A. T. (2003). Use of Speech-Generating Devices: In Support of Natural Speech. Augmentative and Alternative Communication, 19(1), 29-35.
[5] National Institute on Deafness and Other Communication Disorders. (2023). Minimally Verbal/Non-Speaking Individuals With Autism: Research Directions for Interventions to Promote Language and Communication. Virtual Workshop, January 24-25, 2023.
[6] Binger, C., & Light, J. (2007). The Effect of Aided AAC Modeling on the Expression of Multi-Symbol Messages by Preschoolers who use AAC. Augmentative and Alternative Communication, 23(1), 30-43.
[7] Shane, H. C., Laubscher, E., Schlosser, R. W., Fadie, H. L., Sorce, J. F., Abramson, J. S., Flynn, S., & Corley, K. (2015). Enhancing Communication for Individuals with Autism: A Guide to the Visual Immersion System (1st ed.).
[8] Strand, E. A. (2020). Dynamic Temporal and Tactile Cueing: A Treatment Strategy for Childhood Apraxia of Speech. American Journal of Speech-Language Pathology, 29(1), 30-48.
[9] Chenausky, K. V., Norton, A. C., Tager-Flusberg, H., & Schlaug, G. (2022). Auditory-motor mapping training: Testing an intonation-based spoken language treatment for minimally verbal children with autism spectrum disorder. Annals of the New York Academy of Sciences, 1515(1), 266-275.
[10] AssistiveWare. (n.d.). Follow Their Lead: How to Be a Respectful Communication Partner. Retrieved from https://www.assistiveware.com/learn-aac/follow-their-lead-how-to-be-a-respectful-communication-partner.
[11] Niemeijer, D., & Sheldon, E. (2024, October 21). Introducing Proloquo and Proloquo Coach - the next generation of AAC. AssistiveWare Blog. Retrieved from https://www.assistiveware.com/blog/introducing-proloquo-proloquo-coach.
Join the Tech For Talking Special Interest Group
Help shape the future of speech development technology for autistic children
What You'll Get
-
•Group meetings with like-minded professionals and parents
-
•Subsidized and early access to Tech For Talking apps in exchange for participation
Why Join Us
-
•Connect with others passionate about helping autistic children
-
•Be part of meaningful change in speech development technology